HIV represents an unprecedented pandemic that is forcing civil society to innovate in order to meet the challenges. These actors have borrowed advocacy language and techniques from other sectors and regions, conducting the most vocal, widespread and innovative health advocacy to date. HIV activists are at the vanguard of the expansion of human rights discourse into health advocacy, drawing on rights instead of more traditional frameworks like development or public health, even in settings where rights are understood as foreign and confrontational.
In my recent book I focus on sub-Saharan Africa, the region of the world hardest hit by the pandemic, and ask: why do civil society advocacy groups working on HIV choose to express their claims in the language of human rights? How do they understand this choice? What impact do they see it having? The answers might surprise some: the decision to use rights was fueled by individual belief not donor demand and, less than their legal effect, it was the individual empowerment of rights-talk that activists felt was the most important impact.
I examined nine local civil society organizations selected from four countries (Ghana, Uganda, South Africa, Botswana) in three sub-regions of sub-Saharan Africa (West Africa, East Africa, Southern Africa). This breadth provides insight into civil societies operating in different contexts, and at different levels (local, national, regional). In order to allow for a systematic comparison, I chose organizations that vary in the extent to which they use human rights in advocacy. The case studies draw on 145 semi-structured interviews conducted with these organizations, as well as with others linked to their work, and researching relevant events, documents and press accounts.
Over the past twenty years many funders have embraced the human rights framework. While my research does not dispute the importance of largely international donors, it finds that donor demands were not particularly influential on an organization’s choice to use rights-based advocacy. The groups most attached to this framework didn’t lose interest when it dipped in donor popularity, and this interest did not appear to rise or decline in prominence with changes in funding. Organizations at both ends of the rights-spectrum share donors. Also, most groups have at least a dozen donors, and these funders usually support particular projects rather than the organization as a whole. A single donor rarely influences the overall framework an organization chooses for its advocacy.
Rather, I argue that organizations choose human rights primarily due to internal features, highlighting a combination of principled and structural factors. The ideal set of conditions for an organization to choose a rights-based framework includes a leader with a strong human rights orientation, and, where rights are not a dominant national discourse, a centralized organizational structure that allows for regular interaction with other employees. In settings where human rights are not a common discourse, groups manage to thrive even in isolation with powerful “rights champion” leaders. Such leaders are able to incubate a rights-oriented organizational culture, subsequently attracting personnel who have, or will acquire a similar orientation.
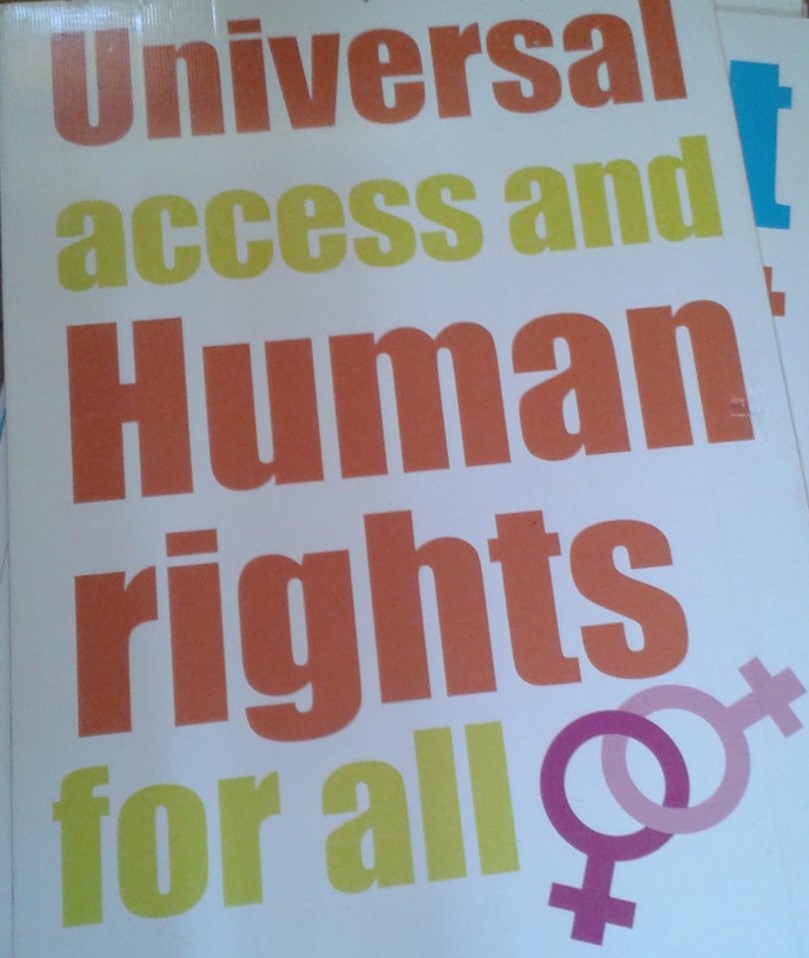
.jpg)
Rights dominant groups often used advocacy materials highlighting human rights. Photo taken with permission by Kristi Kenyon at the Botswana Network on Ethics, Law and HIV/AIDS (BONELA). All Rights Reserved.
Within groups that made dominant use of human rights in advocacy, a strong personal belief in the rights framework was typical. Respondents often explained their own use of human rights in terms of belief—frequently giving lengthy, passionate responses describing human rights as core to their dignity and identity. One participant explained her organization’s use of rights in the following manner:
Your dignity is what will make the world. Dream…. Because dignity is human rights. It’s inherent to existence as a human being. Without it imagine being treated like mud.
[W]ith this respect with human rights really you can never go wrong. Human rights are the reason why we exist, right? … You have those rights, no matter how silent they are, that need to be respected. People should not trample you like a doormat. Your dignity is what will make the world. Dream…. Because dignity is human rights. It’s inherent to existence as a human being. Without it imagine being treated like mud.
Instead of a topic or technique, human rights were understood as a broad and inclusive worldview based on strong belief—almost akin to a secular religion.
I expected that groups would choose rights over other terminology because human rights are tied to legal enforcement in ways that development or public health are not. I thought perhaps the choice to use human rights was rooted in an expectation of government response and legal accountability. Instead, respondents saw the most important impact of human rights as individual-level empowerment of those seeking health care. They saw rights as a framework which empowers those living with HIV to demand services owed to them, and to make requests from a position of power and entitlement, rather than weakness and desperation.
One respondent described the shift in mindset, that she viewed as accompanying rights-based advocacy, as “creating in people’s minds” the idea that they “have the right to demand better.” Respondents gave accounts of these demands: “When you say, ‘It’s my constitutional right, doctor. I am not going to leave this room without having treatment,’ therefore the doctor will make sure that you get the treatment […] They don’t make a mistake.”
While the above quotation is from South Africa, where health rights are included in the Constitution, respondents in settings without such legal codification gave very similar accounts. They saw rights language as transforming people from passive recipients of care to active participants engaged in their own health, and as engaged citizens rightfully demanding services from the state.
This research indicates that “human rights” may yield important effects in places human rights scholars seldom look. Beyond state actions and high-profile venues such as the United Nations and national courts, people are wielding human rights in their day-to-day interactions in ways that have meaningful influence on their lives. The research suggests that human rights-based advocacy has a unique impact in that it changes self- perceptions of power in relation to the state and enables people to claim services to which they are entitled from a position of strength. Those exposed to human rights-based advocacy were reportedly more likely to seek health care services, to be informed about their rights, to ask questions of health care providers, and to query delays or denials of service.
These findings may also have implications for public health, as the ways in which human rights are reported to change behaviour also suggest that human rights-based activism could be an overlooked positive determinant of health.